আমাদের ডিসকাশন ক্লাশ এর সূচী- সকাল ৬.৩০ (রমাদানে- দুপুর ২-৩টা)
শনিবারঃ বিষয়ঃ প্যাথলজি; মঙ্গলবারঃ - বিষয়ঃ অর্গানন অব মেডিসিন; বুধবারঃ বিষয়ঃ- মেটেরিয়া মেডিকা /প্র্যাক্টিস অব মেডিসিন;

Note-1:Blood CBC with ESR/ ব্লাড সিবিসি এবং ই এস আর
Blood CBC
সিবিসি (cbc test) টেস্ট মানে হচ্ছে, Complete Blood Count।এটি একটি স্ক্রিনিং টেস্ট যার দ্বারা শরীরের বিভিন্ন ইনফ্লামাটরি ডিজিস ও ডিসঅর্ডার ডায়াগনোসিস
করা হয়।এটি একটি সিম্পল কিন্তু সেনসিটিভ টেস্ট।ডাক্তার এর মাধ্যমে কিছু রোগ সরাসরি ডায়াগনোসিস করেন,আর কিছু রোগের ব্যাপারে পর্যবেক্ষণ করেন।
# যে কোন ইনফেকশানজনিত ও সিস্টেমিক রোগের জন্য এটি খুব গুরুত্বপূর্ণ
# রক্তশূন্যতার রোগীদের জন্য এটি খুব দরকারী টেস্ট
# ক্যান্সার রোগীদের ইমপ্রুভমেন্ট পর্যবেক্ষণ করার জন্য
# কিছু কিছু ঔষধ রোগীর রক্ত কণিকায় পরিবর্তন নিয়ে আসে।সেটা পর্যবেক্ষণ করার জন্য
# Hb% (Hemoglobin)
# Total RBC (Red Blood Corpuscel) Count
# Total WBC Count
2)eosinophil
3)lumphocyte
4)monocyte
5) basophil
# Total Platelet Count
# PCV /Haematocrit
# MCH
# MCV
# MCHC
# Red Cell Distribution Width(RDW)
# Reticulocyte Count
ই এস আর টেস্ট (ESR test) কি ?
ESR অর্থ Erythrocyte Sedimentation Rate (ESR full form in medical)। ই এস আর টেস্ট(ESR) একটি ডায়াগনস্টিক টেস্ট,এটি রক্ত থেকে করা হয়। এটি CBC বা সিভিসি টেস্ট প্রোফাইলের অনেক গুলো প্যারামিটার থেকে একটি প্যারামিটার।কোন স্পেশাল রোগের জন্য এটি প্রেসক্রাইভ করা হয় না।
এটি মূলত ইন্ডিকেটর হিসেবে ব্যবহার করা হয়।এই টেস্ট ডাক্তারকে কোন একটি রোগের ব্যাপারে সিদ্ধান্ত নিতে সাহায্য করে
কখন ই এস আর টেস্ট(ESR Test) করতে বলা হয়:
ESR Test Normal Range (ই এস আর এর নরমাল ভ্যালু) : 0-10 mm in 1hr (male); 0-20 mm in 1hr (female)
ইএসআর এর প্রকারভেদ / Type of ESR:
যেসব রোগে ই এস আর/ ESR কমে যায়:
যেসব রোগে ই এস আর/ ESR বেড়ে যায়:
যেসব কারণে রোগ ছাড়াই ESR বেশী রেজাল্ট আসে:
Note-1.2:Blood CBC : Hemoglobin/ হিমোগ্লোবিন (রঞ্জক পদার্থ)
Hemoglobin/ হিমোগ্লোবিন (রঞ্জক পদার্থ)
হিমোগ্লোবিন একটি অক্সিজেনবাহী লৌহসমৃদ্ধ মেটালোপ্রোটিন যা মেরুদণ্ডী প্রাণিদের লোহিত কণিকা এবং কিছু অমেরুদণ্ডী প্রাণির কলায় পাওয়া যায়। স্তন্যপায়ী প্রাণিদের ক্ষেত্রে লোহিত রক্তকণিকার শুষ্ক ওজনের ৯৬-৯৭%ই হয় হিমোগ্লোবিনের প্রোটিন অংশ, এবং জলসহ মোট ওজনের তা ৩৫%।
হিমোগ্লোবিন এর কাজঃ
# হিমোগ্লোবিন ফুসফুস হতে অক্সিজেন দেহের বাকি অংশে নিয়ে যায় এবং কোষীয় ব্যবহারের জন্য অবমুক্ত করে।
# এটি অন্যান্য গ্যাস পরিবহনেও অবদান রাখে, যেমন এটি কোষকলা হতে CO2 পরিবহন করে ফুসফুসে নিয়ে যায়।
# প্রতি গ্রাম হিমোগ্লোবিন ১.৩৬ হতে ১.৩৭ মিলিলিটার অক্সিজেন ধারণ করতে পারে, যা রক্তের অক্সিজেন পরিবহন ক্ষমতা ৭০গুণ বাড়িয়ে দেয়।
| প্রোটিনের ধরণ | ক্রিয়া | সহউৎপাদক |
|---|---|---|
| metalloprotein, globulin | oxygen-transport | heme |
| উপএককের নাম | জিন | ক্রোমোজমাল লোকাস |
| Hb-α1 | HBA1 | Chr. 16 p13.3 |
| Hb-α2 | HBA2 | Chr. 16 p13.3 |
| Hb-β | HBB | Chr. 11 p15.5 |
Report: hb% Result: 10; ref value: M-12-16, F-11.0-15.5 g/dl
আরও দেখুন উইকিপিডিয়াNote-1.3:Total RBC Count/ মোট লোহিত রক্ত কণিকা
Total RBC Count/ মোট লোহিত রক্ত কণিকা
RBC গণনা হলো রক্ত পরীক্ষার একটি উপাদান যেখানে আপনার দেহে কি পরিমান লোহিত রক্ত কণিকা আছে তা পরিমাপ করা যায়।
লোহিত রক্ত কণিকাতে যা আছে :
# RBC count সব সময় complete blood count (CBC) test এর একটা অংশ।
# এই পরীক্ষা বিভিন্ন প্রকারের এনিমিয়া (low number of RBCs) এবং অন্যান্য বিষয় যা লোহিত রক্ত কণিকায় প্রভাব ফেলে।
RBC count এ যে সকল বিষয় পাওয়া যাবে
# (Waldenstrom macroglobulinemia) শ্বেত রক্ত কণিকার ক্যান্সার।
# (paroxysmal nocturnal hemoglobinuria) ডিজঅর্ডার যা লোহিত রক্ত কণিকাকে স্বাভাবিক অবস্থা থেকে সময়ের আগেই ভেঙ্গে ফেলে।
# (myelofibrosis) Bone marrow disorder বা মেরুমজ্জার ডিজঅর্ডার যেখানে মেরুমজ্জা স্কার (scar tissue) টিস্যু দ্বারা পরিবর্তন হয়।
RBC এর স্বাভাবিক রেঞ্জ
# মহিলাঃ ৪.২ - ৫.৪ মিলিয়ন সেল প্রতি মাইক্রোলিটার (cells/mcL)
# উপরোক্ত ভ্যালু হচ্ছে সাধারণ কমন ভ্যালু , এটা বিভিন্ন কোম্পানীর রি-এজেন্টের উপর নির্ভর করে।
RBC এর অস্বাভাবিক ফলাফলঃ নরমাল ফলাফলের চেয়ে উচ্চ ফলাফল প্রদর্শিত হয়, এর জন্য যে সকল কারণ সমুহ দ্বায়ী-
# হৃৎপিণ্ডের (heart's) সমস্যা (গঠন ও কার্যক্রম ) যা জন্ম থেকেই হয়ে থাকে।
# হৃৎপিণ্ডের (heart's) ডান পার্শ্বের ফেলিউর (cor pulmonale)।
# পানিশুন্যতা (যেমনঃ মারাত্বক ডায়েরিয়া)।
# কিডনীর টিউমার (renal cell carcinoma)।
# রক্তের অক্সিজেন লেভেল এর নিম্বতা বা ঘাটতি (hypoxia)
#ফুসফুসে দাগ বা ফুসফুসের তন্তুময় টিউমার (pulmonary fibrosis)।
# বোন মেরো বা হাড়ের মেরুমজ্জায় সমস্যা যা RBCs অস্বাভাবিকভাবে বেড়ে যায়, (polycythemia vera)
# উচ্চ চাপে বা উচ্চ স্থানে গেলে কয়েক সপ্তাহ পর্যন্ত RBCsবেড়ে যেতে পারে।
যে সকল ঔষধ RBC count অস্বাভাবিক ভাবে বাড়িয়ে দেয়ঃ
# Methyldopa
যে সকল ঔষধ RBC count অস্বাভাবিক ভাবে কমিয়ে দেয়ঃ
#ক্লোরামফেনিকল ( Chloramphenicol)
# হাইডানশন (Hydantoins)
# কুইনাইডাইন (Quinidine)
RBC এর ফলাফল (count) যে সকল কারণে নিম্ন হয়ঃ -
# অতিরিক্ত রক্তক্ষরণ ( Bleeding)
# বোন মেরো বা মেরুমজ্জার কার্যক্রম বন্ধ হয়ে যাওয়া - যেমনঃ বিকিরণ (radiation), বিষ (toxins) অথবা টিউমার ।
# হরমোন ডিফিসিয়েন্সি যেমন ইরিথ্রোপোইয়েটিন ( erythropoietin- caused by kidney disease)
# RBC destruction বা ভেঙ্গে যাওয়া (hemolysis- ট্রান্সফিউশন, ব্লাড ভেসেল ইনজুরি অথবা অন্যান্য কারণে ঘটে ।
# লিউকোমিয়া
# ম্যালনিউট্রেশন
# বোন ম্যারো ক্যান্সার (multiple myeloma)
# দৈনন্দিন খাবারে খুব নিম্ন মাত্রার আয়রণ, কপার, ফলিক এসিড, ভিটামিন বি৬ অথবা ভিটামিন বি১২ ।
# অতিরিক্ত পরিমাণে পানি পান করা।
# গর্ভকালীন সময়।
Risks
There is little risk involved with having your blood taken. Veins and arteries vary in size from one person to another and from one side of the body to the other. Taking blood from some people may be more difficult than from others.
Other risks associated with having blood drawn are slight, but may include:
# Fainting or feeling lightheaded
# Multiple punctures to locate veins
# Hematoma (blood buildup under the skin)
# Infection (a slight risk any time the skin is broken)
References
# Bunn HF. Approach to the anemias. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 25th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 158.
# Chernecky CC, Berger BJ. Red blood cell (RBC) – blood. In: Chernecky CC, Berger BJ, eds. Laboratory Tests and Diagnostic Procedures. 6th ed. Philadelphia, PA: Elsevier; 2013:961-962.
Note-1.4:Blood CBC : Total WBC Count
Total WBC Count/ শ্বেত রক্তকণিকার গণনা
শ্বেতকণিকা
শ্বেতকণিকা (ইংরেজি: White blood cell or Leucocytes) মানবদেহে রক্তের একটি উপাদান। রক্তে বর্ণহীন, নিউক্লিয়াসযুক্ত এবং তুলনামূলকভাবে স্বল্পসংখ্যক ও
বৃহদাকার যে কোষ দেখা যায় এবং যারা দেহকে সংক্রমণ থেকে রক্ষা করতে সাহায্য করে তাকে শ্বেতকণিকা বলে। প্রাপ্তবয়স্ক মানুষের দেহে শ্বেত রক্তকণিকার সংখ্যা প্রতি ঘন
মিলিলিটারে ৪০০০-১১০০০(গড়ে ৭৫০০)। লোহিতকণিকার তুলনায় শ্বেতকণিকার সংখ্যা অনেক কম। লোহিতকণিকা ও শ্বেতকণিকার অনুপাত প্রায় ৬০০:১। রক্তে শ্বেতকণিকার সংখ্যা
স্বাভাবিকের চেয়ে বেশি থাকলে তাকে লিউকোসাইটোসিস বলে এবং কম থাকলে তাকে লিউকোপেনিয়া বলে। লিউকেমিয়া ক্যান্সারের ক্ষেত্রে শ্বেত রক্তকণিকার সংখ্যা অস্বাভাবিক
হারে বেড়ে যায়[১] শ্বেত রক্ত কণিকার আয়ু ১-১৫ দিন, এরপর সাধারণত কোষগুলো ধ্বংস প্রাপ্ত হয়।
প্রকারভেদঃ গঠনগত ভাবে এবং সাইটোপ্লাজমের দানার উপস্থিতি বা অনুপস্থিতি অনুসারে শ্বেতকণিকাকে দুই ভাগে ভাগ করা যায় যথা:-
শ্বেতকণিকার পরিমাণ ৭২% । নিউক্লিয়াসের আকারের ভিত্তিতে এরা আবার তিন প্রকার। যথা :
# ইওসিনোফিল(Eosinophil): ইওসিনোফিল ও বেসোফিল হিস্টামিন নামক রাসায়নিক পদার্থ নিঃসৃত করে এলার্জি প্রতিরোধ করে।
# বেসোফিল (Basophil):বেসোফিল হেপারিন নিঃসৃত করে রক্তকে রক্তবাহিকার ভিতর জমাট বাধতে বাধা দেয়।
Note-2.1:Cellular Alteration (কোষের পরিবর্তন):
প্রকারভেদ
কোষের উদ্দীপনা অনুযায়ী ক্ষতের প্রকারভেদ (Types of Cellular Alterations in Response to Injury)
A. Cellular Adaptations [কোষীয় অভিযোজন- যখন আমাদের শরীরের কোনো কোষ ক্ষতিকর উপাদানের সম্মুখীন হয়, তখন সেই কোষ নিজের মধ্যে এমন কিছু পরিবর্তন নিয়ে আসে, যাতে ওই ক্ষতিকর আবহেও কোষটি টিকে থাকতে পারে। এই পরিবর্তন গুলিকেই আমরা কোষীয় অভিযোজন বলি। ]:- It is the state between normal cell and the injured cell :
(1) এট্রপি
Atrophy, (2) হাইপারট্রপি
Hypertrophy, (3) হাইপারপ্লাসিয়া
Hyperplasia. (4) মেটাপ্লাসিয়া
Metaplasia .
B. Cell Injury:- কোষের আঘাত বা ক্ষতি এমন একটি অবস্থা যা অভিযোজনের সীমার বাইরে। ক্ষতিকারক এজেন্ট দ্বারা কোষের আঘাত বা কোষের ক্ষতি প্রথমে জৈব রাসায়নিক স্তরে ঘটে।(Cell injury or damage is a state which is beyond the limits of adaptation. Cell injury or cell dam- age by an injurious agent at first occurs at the biochemical level.)
যেমন-
1. Reversible cell injury (degeneration):
2. Irreversible cell injury and cell death
(c) Subcellular Alterations.
D. Intracellular Accumulations.
E. Pathologic Calcification.
F. Hyaline Change.
ননলেথাল ইনজুরি প্রত্যাবর্তনযোগ্য কোষের আঘাত (অবক্ষয়) এবং প্রাণঘাতী আঘাত অপরিবর্তনীয় কোষের আঘাত এবং মৃত্যুর দিকে নিয়ে যায়। কোষের মৃত্যুর পরে নেক্রোসিস বা অ্যাপোপটোসিস হয়। কোষের ক্ষতি ক্ষতিকারক এজেন্টের ধরন, এর সময়কাল এবং তীব্রতার উপর নির্ভর করে। কোষের পরিবর্তন কোষের ধরন এবং এর পুষ্টি, হরমোন এবং বিপাকীয় অবস্থা এবং অভিযোজন ক্ষমতার উপরও নির্ভর করে। Necrosis is one of the two types of morphologic changes Then Tomos cell death in living tissue A necrotic cell cannot reverse back to normal cell Changes of necrosis occur due to (1) Denaturation of proteins. (2) Enzy marks digestion of the cell by (a) Autolysis. Autolysis Is the self digestion of cells after their death. It occurs due to the action of its own enzymes like proteases, li pases, esterases, ribonuclease, deoxyribonuclease mainly derived from lysosomes of the cell. These act at low pH, (h) Heterolysis. It is the digestion of cells by enzymes from lysosomes of immigrant leucocytes. These changes take hours, eg 8 to 12 hours in myocardial infarction
সেল ইঞ্জুরির কারণ
i. Hypoxia.
2. Infectious Agents:- Bacteria, viruses, fungi, protozoa and helminths
3. Immunologic injury:- Hypersensitivity reactions cause cell injury.
4. Physical Agents:- Mechanical trauma, hurn, ionizing, radiation, cold.
5. Drugs and Chemicals:- Alcohol, narcotics, cytotoxic drugs, poisons.
6. Nutritional Imbalance:- Protein energy malnutrition.
7. Genetic defects, eg Inborn errors of metabolism.
8. Aging.
Pathogenesis of Hypoxic (Ischaemic) Cell Injury
A. Reversible cell injury
1 First attack on the oxidative phosphorylation (acrobic respiration) in mitochondria of the cell As oxygen ten- sion decreases within the cell,
there is loss of oxidative phosphorylation and the generation of ATP (Adenosine triphosphate) slows down or stops. Diminished ATP and ATPase leads to failure of 'sodium pump', and thereby active membrane transport. It leads to accumulation of Sodium intracellularly, loss of potassium from cell and accumulation of water causing acute cellular swelling
(cellular oedema).
2. Increased rate of anaerobic glycolysis. AMP (Aden- osine monophosphate) increase stimulates phosphofruc- tokinase and phosphorylase activities. Glycogen is de- pleted, lactic acid and inorganic phosphates accumulate leading to reduction in intracellular pH.
Early dilatation of endoplasmic reticulum. 4. Detachment of ribosomes from endoplasmic reticulum
5. Dissociation of polysomes into monosomes.
6. Mitochondria are swollen.
7. Formation of membrane blebs at the cell surface
8. Myeline figures
may be seen.
9. Clumping of nuclear chromatin.
10. Autophagy by lysosomes.
B. Irreversible cell injury
Profound membrane damage and mitochondrial dys- function are critical events.
1. Cell membrane damage is the earliest change. It is the cirtical change of lethal injury. Mechanisms (a) Pro- gressive loss of phospholipids, (b) Increased calcium in cytosol due to influx, C) Toxic oxygen radicals (Rea- ctive oxygen species) induce injury, (d) Cytoskletal ab- normalities. e) Lipid break- down products, (1) Exit of enzymes-CPK (CK), LDH, and (g Loss of intracellular amino acids.
2. Mitochondria including cristae show severe vacuoliza- ion (High-amplitude swelling).
3. Reduction of intracellular pH leads to intracellular re- ease of lysosomal enzymes with protein digestion.
4. Clumping of nuclear chromatin and nuclear changes.
5. Lipid depositions. Amorphous densities in mitochon- al matrix.
Pathogenesis of Chemical Cell Injury
Cell damage may occur by two mechanisms A. Direct Cytotoxic Effects. It occurs by combining with cellular components These are mostly water solu be chemicals Examples:
2. Cyanide. It directly poisons mitochondrial enzymes
3. Mercuric chloride Mercury binds to the sulphydryl groups leading to the increased membrane permeability and inhibition of ATPase dependent transport
B. By reactive free radicals and lipid peroxidation These are mainly lipid-soluble toxins, eg;. carbon tetra- chloride The enzyme P-450 converts CCI4 to highly re- active toxic free radical CCI3 which leads to lipid per- oxidation.
Cell Injury by Free Radicals: Free radicals are chemical species that have a single unpaired electron in an outer orbit. Important free radicals:
(2) Nitric oxide (NO) It can act as free radical and can also produce reactive peroxynitrite anion (ONOO-) NO 2 - and NO3-,
(3) CCI3, a free radical derived from CCI4
Production site of free radicals in cells.
These may be produced in plasma membrane, lysosomes, mitochondria and cytosol of the cell by oxidative enzymes Initiating factors are:
(2) Radiant energy like ultraviolet rays, X-rays,
(3) Metabolic product of drugs or chemicals, eg CCI3.
Initiation- Propagation due to further formation of free radicals.
Effects: Free radicals play role in:-
(1) Microbial killing by phagocytic cells, (2) Inflammatory damages, (3) Chemical injury to cells, (4) Radiation injury. (5) Cellu- lar aging. (6) Destruction of tumour cells by macrophages, and (7) Other reactions.
Mechanisms of actions of free radicals in cellular injury are:
(a) Lipid peroxidation of membranes, (b) Damage to DNA, (c) Oxidative modification of proteins.
Inactivation of free radicals may occur by
(1) Antioxi- dants, eg vitamin E, serum albumin, transferrin and ceruloplasmin, cysteine, glutathione, (2) Enzymes- su- peroxide dismutase, catalase, glutathione peroxidase.
Mechanisms of Cell Injury with Other Injurious Agents
2. Physical Agents: These cause direct cell damage- re- versible or irreversible injury and death. Ionizing radia- tion can produce free radicals which cause cell damage.
REVERSIBLE CELL INJURY:
Types
Under light microscope, the morphologic changes are mostly confined to the cytoplasm. The nucleus shows no change.
1. Cellular Swelling
2. Fatty change ( see previous)
Fates of Reversible Cell Injury
1. Reverse to normal cell
2. Injury persists in reversible state
3. Passes to irreversible injury and death
NECROSIS
Morphology. Microscopic changes
(1) Nuclear changes. Under light microscope, nuclear changes are the hallmark of necrosis It takes one of the three pat- terns (a) Pyknosis. The nucleus is shrinked, condensed and more basophilic DNA is condensed into a solid, ba- sophilic mass, (b) Karyorrhexis. Pyknotic nucleus breaks up into fragments, (c) Karyolysis. Basophilia of the chromatin fades due to DNAse activity. In a day or two the nucleus totally disappears. (2) Cytoplasm. More glassy, eosinophilic, homogeneous and vacuolated in ap- pearance than normal cells. (3) The cell swells with loss of demarcation and contour Ultramicroscopic changes are described under pathogenesis of irreversible injury
Types of Necrosis A. Basic Types of Necrosis
W. Coagulative Necrosis. This results from denaturation of structural and enzymic proteins. The basic cellular shape, cell outlines and tissue architecture is maintained. This is structured necrosis. The cell takes acidophilic stain. Examples Hypoxic death of cells in all tissues except brain, eg infarct of heart, kidney, spleen. Histol- ogy of myocardial infarct-See chap 22, slide 16. (b) Gumma of tertiary syphilis. It has gummy consistency. The necrotic zones are usually surrounded by inflamma- tory cells.
2. Liquefactive or Colliquative Necrosis. This results
from autolysis or heterolysis by the action of powerful
catalytic enzymes. Liquefactive necrosis occurs in: (
Suppurative or purulent inflammation.
slide Hypoxic death of cells within brain - Infarction of brain. There occurs softening of the necrosed.
It then breaks up and turns into fluid. There may be cyst formation. Cascous material as secondary change.
B. Other Types of Necrosis
1. Caseous Necrosis. This is à distinctive type of coagu- lative necrosis. It occurs most commonly in the tuberclePATHOLOGY fa lesion of tuberculosis). The architecture is lost and the cell outlines are not preserved. There is Tormation of "Son Trable, amorphous granular debris resembling Cheesy material.jeascous Liquefaction i cascous ma terial may occur The area is surrounded by granuloma tous inflammatory cells. See chap slide
2. Fat Necrosis. It occurs in adipose tissue due to action of lipase
(b) Traumatic fat necrosis. It occurs usually in the breast. The necrosed area may be surrounded by in nammatory changes with accumulation of neutrophils, Tipid laden macrophages, giant cells and then fibroblasts Finally the area is replaced by scar tissue which may produce skin retraction and clinically may resemble scir-
rhous carcinoma.
3. Fibrinoid Necrosis. It is a morphologic descriptive term of a variety of changes. There is necrosis of collagen Fibrocytes undergo necrosis and its fibres appear to degenerate. In this there is swelling and fragmentation of the collagen fibres. There is fibrinoid deposit which is a smudgy cosinophilic deposit. It is thought to be due to fibrinogen precipitation or fibrin. It occurs in (a) Acute rheumatic fever, due to immune complex mechanism. (b) Connective tissue disorders, eg Theumatoid arthritis, systemic lupus erythematosus, polyarteritis nodosa and other vasculitis due to immune complex mechanism, (c) Arthus phenomenon, (d) Shwartzman phenomenon, and (e) Malignant
hypertension in arterioles.
4. Gangrenous Necrosis- See below under gangrene. Gangrene is necrosis of tissue with superadded putrefac- tion by bacteria.
5. Necrosis of Muscle (Zenker's degeneration). This type of necrosis particularly occurs in rectus abdominis
Note-1.3: Chapter of Kent Repartory ( কেন্ট রেপারটরীর অধ্যায় সমুহ
MVH/ EH/ EV/ Ns/ FMTTE/ SARS/ U-(BKPU)-U/ GmGf/ LtRCE/ CBE/ SdCFP/ SG (AT A GLANCE)
Meaning:
M (Mind), V (Vertigo), H (Head) / E (Ear), H (Hearing)/ E (Eye), V (Vision)/ N (Nose) s (Smell)/ F (Face), M (Mouth), T (Teeth), T (Throat), E (External Thorat)/ S (Stomach), A (Abdomen), R (Rectum), S (Stool)/ U (Urinary Organs),-(B (Bladder), K (Kidnys), P (Prostate Gland), U (Urethra)-U (Urine)/ G (Genetal) m (Male), G (Genitalia) f (Female)/ L (Larynx) t (Trachea) R (Respiration), C (Cough), E (Expectoration) / C (Chest), B (Back), E (Extrimities)/ S (Sleep) d (Dream)C (Chill), F (Fever), P (Perspiration)/ S (Skin), G (Generalities)
Note: Dr.Tarik zamil: কেন্ট রেপার্টরিতে যে কয়টি সাব অঙ্গ রয়েছে নিন্মে তা দেওয়া হলো।
-১৪ টি সাব অঙ্গ এর অধায়ঃ-
H/E/E/N/F/M/M/T/B/C/A/G/G/E EGG of HEN Corporation FEMAs for BTMC
Meaning:
H (Head) / E (Ear)/ E (Eye)/ N (Nose)/ F (Face)/ M (Mouth)/ M (Mouth Glands)/ T (Teeth)/ B (Back)/ C (Chest)/ A (Abdomen)/ G (Genetal)/ G (Genitalia)/ E (Extrimities)
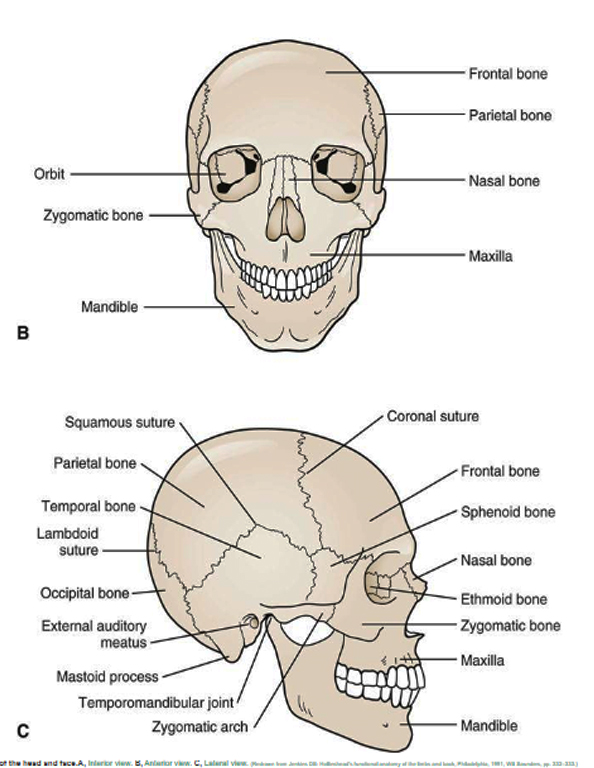
HEAD--৭ টি সাব অঙ্গ।
********************
1. Forehead. কপাল,সামনের অংশ।
2.Temporal.কানের উপরের হাড়।(২টি)
3.Parietal.মধ্যকপালি।
4.Occiput.---পিছনের হাড়।
5. Vertex.তালু।
6.Brain.---মস্তক।
7.Bone.----অস্থি।

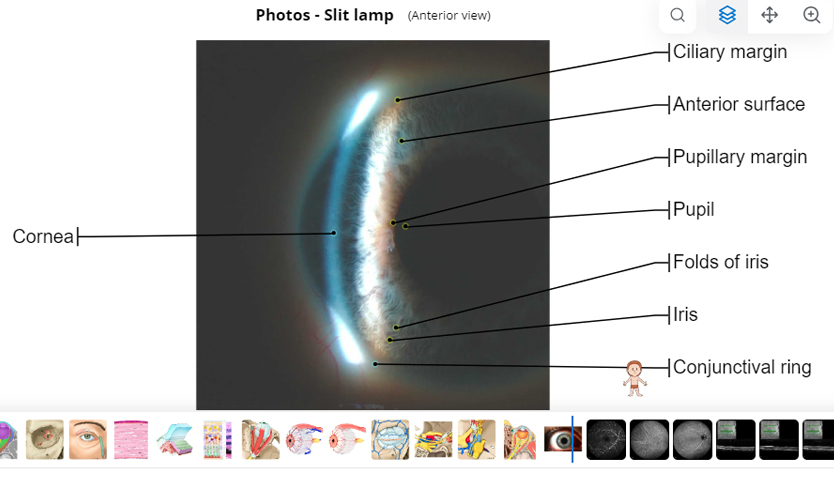
EYE--৩ টি সাব অঙ্গ।
********************
1.Conjunctive.চোখের সাদা অংশ।
2.Cornea.---চোখের কালো অংশ।
3.Orbital fossa.----চোখের গর্ভ।
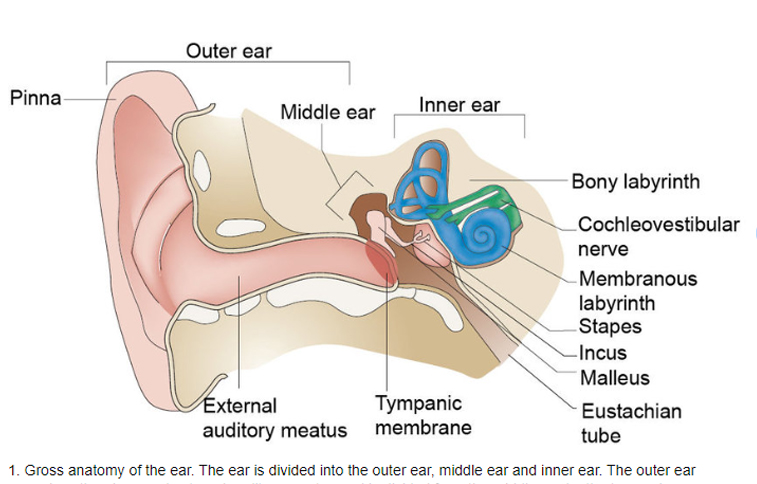
EAR- ২ টি সাব অঙ্গ।
********************
1.Pinna.--কানের বাহির অংশ।
2.External acoustic meats.----কানের কর্তগুহ্বর।
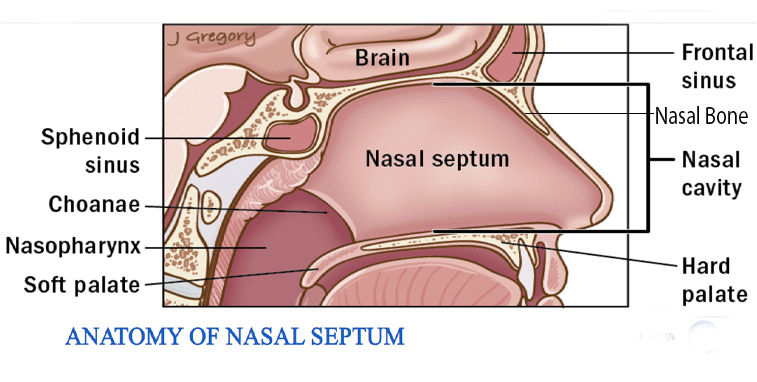
Nose--২ টি সাব অঙ্গ।
********************
2.Nasal Cavity.---নাকের ফাকা অংশ।
FACE-৬ টি সাব অঙ্গ।
********************
1. Zygomatic.---মুখের উচু হাড়।
2.Chin-----.থুতনি।
3.Parotid gland.---মামস, লালা গ্রন্থি, কানের নিচের গ্রন্থি।
4.Maxilla.----উপরের চোয়াল।
5.Mandible.---নিচের চোয়াল।
6.Jaws---.চোয়াল।
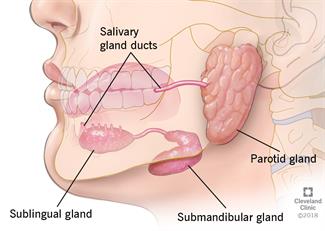
MOUTH GLAND-- ৩টি সাব অঙ্গ।
********************
1.Parroted gland.-- লালা গ্রন্থি।
2.Sub maxillary gland-maxillary bone.---এর সাথে যে গ্রন্থি থাকে।
3.Sublingual glad.--.জিহ্বার নিচের গ্রন্থি।
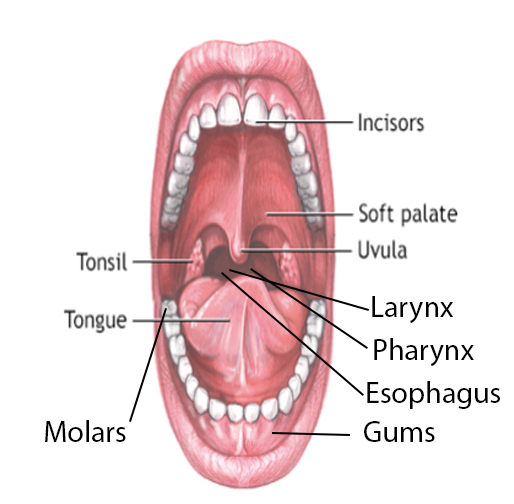
MOUTH--৮ টি সাব অঙ্গ।
********************
1.Uvula.----আল-জিহ্বা।
2.Tonsils.--- টনসিল।
3.Larynx.---শ্বাসযন্ত্রের পথ
4.Pharynx---শ্বাস ও খাদ্য নালীর পথ।
5.Esophagus.---খাদ্য নালী।
6.Gums-মাড়ি।
7Palate-- --মুখের তালু।
8.Molars---.মাড়ির দাঁত।
TEETH - ৫ টি সাব অঙ্গ।
********************
1.Incisors.---কর্তন দাঁত।
2.Cabins.--শ্বাদন্ত।
3.Molars. ---চর্বন দাঁত।
4.Premolars.--চর্বন দাঁত।(প্রায়)
5.Caries.--দাঁত ক্ষয়।

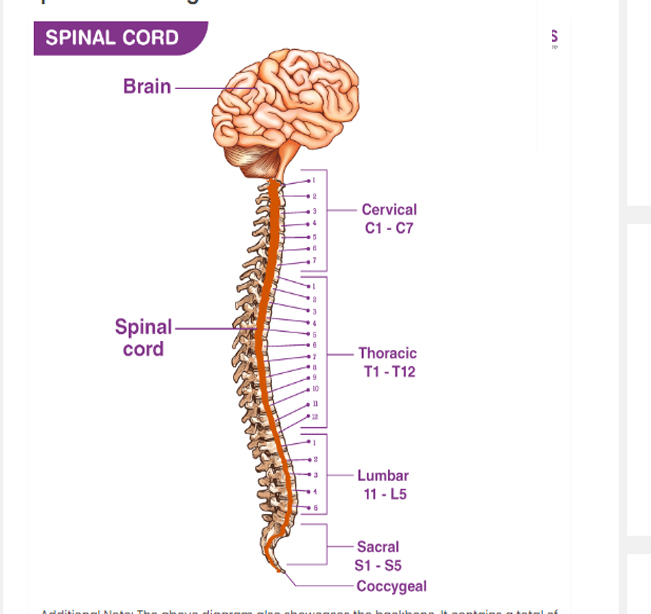
BACK--৮ টি সাব অঙ্গ।
********************
1.Cervical (C1-C7) ৭ টি হাড়।
2.Dorsal (T1-T12)---১২ টি পিঠের পিছনে।
3.Lumber(L1-L5)--৫টি পেট বরাবর।
4.Sacrum(S1-S5)--৫টি কোমড়ে
5.Coccyx(C1-C4)---৪ টি কোমড়ের নিচে।
6.Scapulae (S1-S2)--২ টি ত্রিকোনাস্থি।
7.Spinal Cord---মেরুমজ্জা।
8.Spin.--- মেরুদন্ড।
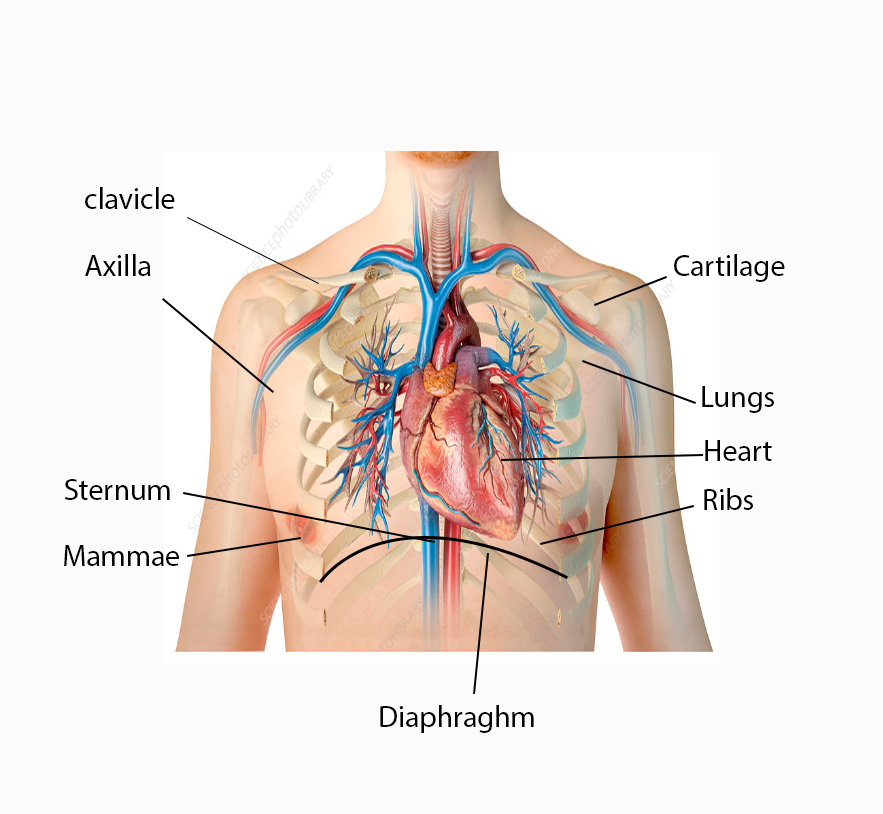
CHEST---৯ টি সাব অঙ্গ।
**********************
1.Clavicle.ঘাড়ের নিচের হাড়।
2.Axilla.---বগল।
3.Sternum------দুই পাঁজরের মাঝের হাড়।
4.Ribs------পাজরের হাড়।
5.Lungs.---ফুসফুস।
6.Heart.---হৃদপিন্ড।
7.Diaphragm ---পেট ও বুকের মাঝের পর্দা।
8.Mammae.---স্তন।
9.Cartilage.----তরুণাস্থি।
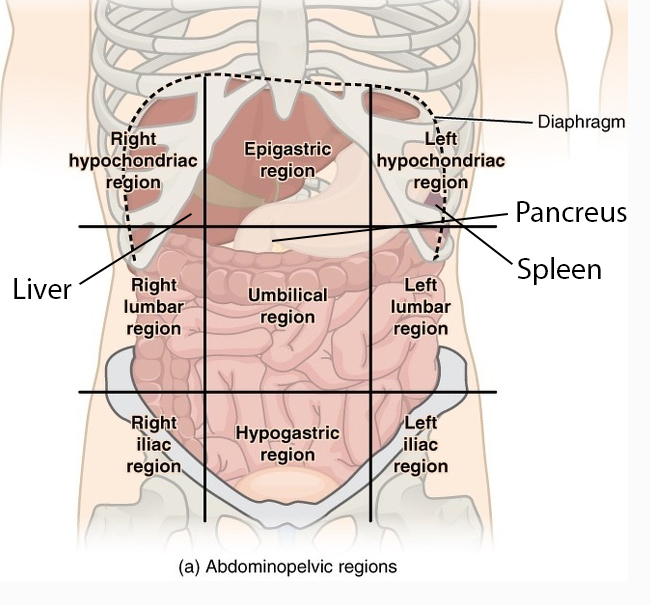
ABDOMEN--- 12 টি সাব অঙ্গ।
**********************
1.Liver (যকৃৎ)
2.Spleen (স্প্লিন)
3.Pancreus (অগ্নাশয়)
Abdomen Region (9)
2.Left Hypochondrium.
3.Epigastic.
4.Hypogastic
5.Umbilicus
6.Right Lumber
7.Left Lumber.
8.Right iliac
9.Left iliac.
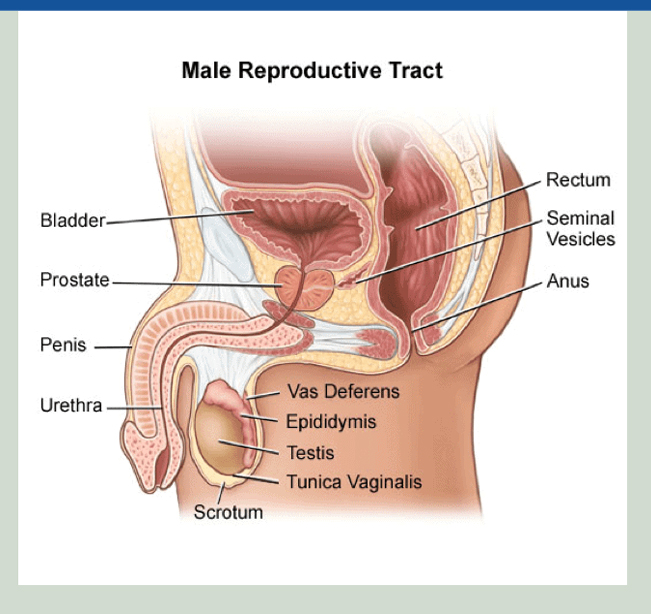
GENITALIA--- ৬ টি সাব অঙ্গ।
**********************
1.Penis.--লিঙ্গ।
2.Scrotum.--অন্ডথলি।
3.Spermatic Cord.শুক্রবাহী নালী।
4. Testes.--অন্ডকোষ।
5. Bladder.--মূত্র থলী।
6. Mixed gland-(Testes and Pencreus)
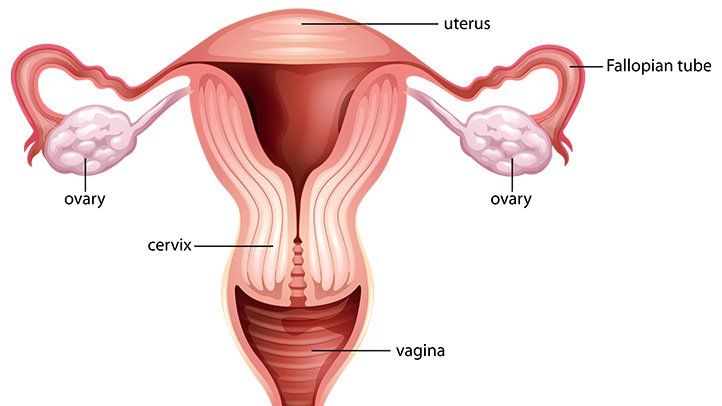
GENITALIA FEMALE --৪ টি সাব অঙ্গ।
**********************
2. Vagina.--স্ত্রী লিঙ্গ।
3.Overies--ডিম্বকোষ।
4. Placenta tained.--গর্ভফুল।
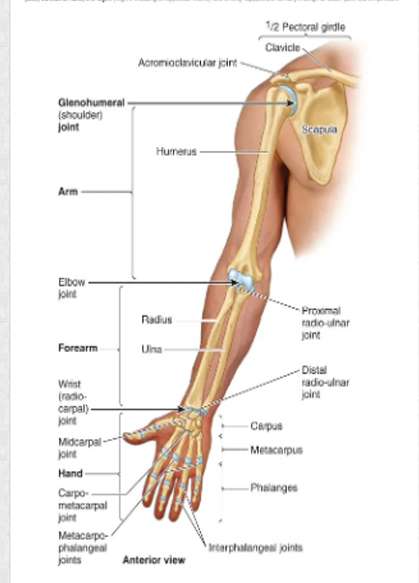
EXTREMETIES
Upper limbs--১২ টি সাব অঙ্গ।
**********************
1.Upper arm.-উর্ধ্ব ভাগ।
2. Hand.--হাত।
3. Humerus.--লম্বা অস্থি।
4. Elbow---কনুই।
5.Forearm--কনুইর নিচের অংশ।
6.Wrist---কব্জি।
7.Fingers---আঙ্গুল।
8.Nails.---নখ।
9.Tips.--আঙ্গুলের অগ্রভাগ।
10.Thumbs.--বৃদ্ধা আঙ্গুল।
11.Sholder.---কাঁধ
12.Plum.--হাতের তালু।
Lower limbs--১৪ টি সাব অঙ্গ।
**********************
1.Hip- কোমর।
2.Sciatica-- কোমর থেকে পা পর্যন্ত স্নায়ু।
3.Femur.- দীর্ঘ অস্থি।
4 Patella. --হাটুর অস্থি।
5. Tibia.-- পায়ের সামনের অস্থি।
6.Fibula.--পায়ের পিছনের অস্থি।
7.Foot.--পায়ের পাতা।
8.Knee.--হাটু।
9.Leg.--পা।
10.Calf--পায়ের ডিম।
11.Ankle--গোড়ালী।
12.Heel.--গোড়ালীর নিচের অংশ।
13.Toes.--পায়ের আঙ্গুলের অগ্রভাগ।
14. Pariosteum- অস্তিত্ব আবরণ।
Note-2.1: কাতরতা:
কাতরতা "#গরমকাতর" এবং "#শীতকাতর" — এই দুটি শব্দ হোমিওপ্যাথি চিকিৎসাপদ্ধতিতে রোগীর ধাতুগত প্রকৃতি ( #Constitution) বোঝার জন্য অত্যন্ত গুরুত্বপূর্ণ। সহজ কথায়, এই শব্দ দুটি দ্বারা বোঝানো হয় একজন ব্যক্তি গরম নাকি ঠান্ডা আবহাওয়ায় বেশি কষ্ট পান এবং কোন পরিবেশে তিনি আরাম বোধ করেন। 💠 #গরমকাতর (#Hot #Patient) 🌹সংজ্ঞাঃ গরম কাতর হলেন সেই ব্যক্তি যিনি গরম আবহাওয়া বা উষ্ণতা একেবারেই সহ্য করতে পারেন না এবং ঠান্ডা পরিবেশে থাকতে পছন্দ করেন। 🌹সাধারণ বৈশিষ্ট্য: 💚 #গরম অসহ্য: গ্রীষ্মকাল বা গরম আবহাওয়া এদের জন্য খুব কষ্টকর। 💚 #ঠান্ডা পছন্দ: এরা সবসময় ঠান্ডা পরিবেশ, ঠান্ডা জল, ঠান্ডা খাবার বা পানীয় পছন্দ করেন। 💚 #ফ্যান/এসি অপরিহার্য: ফ্যান বা এসি ছাড়া থাকতে পারেন না। অল্প গরমেও তাদের শরীর অত্যধিক উত্তপ্ত হয়ে ওঠে। 💚 #খোলামেলা পরিবেশ: বদ্ধ ঘরের চেয়ে খোলামেলা জায়গায় বা জানালার পাশে থাকতে ভালোবাসেন। 💚 #গরম পোশাক অপছন্দ: শীতকালেও মোটা বা গরম জামাকাপড় পরতে চান না। 💚 #সহজে ঘামেন: অল্প পরিশ্রমে বা সামান্য করতে ভালোবাসেন। 🩺উদাহরণঃ একজন গরম কাতর ব্যক্তি শীতকালে হয়তো একটি পাতলা চাদর গায়ে দেবেন, যেখানে অন্যেরা মোটা কম্বলের নিচে থাকবে। 💠 শীতকাতর ( #Chilly #Patient) 🌹সংজ্ঞা: শীতকাতর হলেন সেই ব্যক্তি যিনি ঠান্ডা আবহাওয়া বা শীতলতা একেবারেই সহ্য করতে পারেন না এবং উষ্ণ পরিবেশে থাকতে ভালোবাসেন। 🌹সাধারণ বৈশিষ্ট্য: 💚 #ঠান্ডা অসহ্য: শীতকাল বা ঠান্ডা আবহাওয়া এদের জন্য খুব যন্ত্রণাদায়ক। 💚 #গরম পছন্দ: এরা সবসময় উষ্ণ পরিবেশ, গরম জল, গরম খাবার বা পানীয় (যেমন - গরম চা, কফি, স্যুপ) পছন্দ করেন। 💚 #ফ্যান/এসি এড়িয়ে চলেন: এমনকি গরমকালেও সরাসরি ফ্যানের বাতাস বা এসির ঠান্ডা সহ্য করতে পারেন না। 💚 #শরীর ঢাকা রাখতে চান: সবসময় শরীর ঢেকে রাখতে পছন্দ করেন। অল্প শীতেই মোটা জামাকাপড়, মোজা, বা কাঁথা-কম্বল ব্যবহার করেন। 💚 #সহজে কাঁপুনি আসে: অল্প ঠান্ডাতেই তাদের কাঁপুনি দিয়ে জ্বর আসার মতো অনুভূতি হয়।গরম জলে স্নান: শীতকালে তো বটেই, এমনকি গরমকালেও অনেকে ঈষদুষ্ণ জলে স্নান করতে পছন্দ করেন। 🩺উদাহরণঃ একজন শীতকাতর ব্যক্তি হালকা মেঘলা দিনেও বা এসির ঘরে একটি চাদর বা সোয়েটার পরে থাকতে পারেন। হোমিওপ্যাথিতে এর গুরুত্ব হোমিওপ্যাথিতে ঔষধ নির্বাচনের ক্ষেত্রে রোগীর কাতরতা জানা অপরিহার্য। কারণ— 💠 #ধাতুগত প্রকৃতি নির্ণয়ঃ এটি রোগীর সামগ্রিক শারীরিক ও মানসিক গঠন বুঝতে সাহায্য করে। 💠 #ঔষধ নির্বাচনঃ প্রত্যেকটি হোমিওপ্যাথিক ঔষধেরও নিজস্ব কাতরতা থাকে। কিছু ঔষধ প্রধানত গরম কাতর রোগীদের জন্য বেশি কার্যকর, আবার কিছু ঔষধ শীতকাতর রোগীদের ক্ষেত্রে ভালো কাজ করে। 🩺গরম কাতর ঔষধের উদাহরণঃ সালফার (#Sulphur), পালসেটিলা (#Pulsatilla), এপিস মেল (#Apis_Mel), ইত্যাদি। 🩺শীতকাতর ঔষধের উদাহরণঃ আর্সেনিক অ্যালবাম (Arsenic Album), হিপার সালফ (Hepar Sulph), সোরিনাম (Psorinum), ইত্যাদি। 💠 #একজন অভিজ্ঞ হোমিও ডাক্তার রোগীর অন্যান্য লক্ষণের সাথে তার কাতরতার বিষয়টি মিলিয়ে সবচেয়ে উপযুক্ত ঔষধটি নির্বাচন করেন, যা আরোগ্যের পথকে সহজ করে তোলে।
Disclaimer শিক্ষামূলক উদ্দেশ্যে প্রণীত। সহায়তায়ঃ Open AI (Chatgpt, Gimini) বিভিন্ন ধরনের web, Facebook পোস্ট